- +91 75677 63301
- 24*7 Emergency Care

Don't let brachial plexus palsy pain hold you back

Book your consultation

Satisfied Patients
0 +

Brachial Plexus Palsy Surgeries
0 +

Awards
0 +

Years
0 +
Menu
Brachial plexus palsy treatment in Ahmedabad
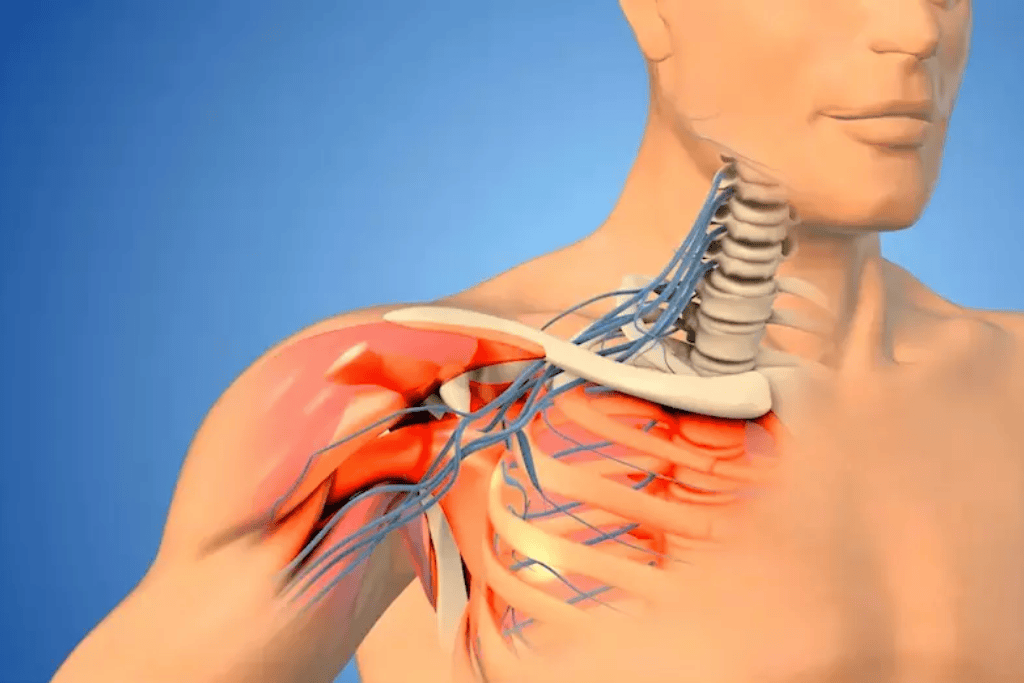
What is brachial plexus palsy?
Brachial plexus palsy refers to a condition where the network of nerves responsible for controlling the muscles and sensation in the arm, shoulder, and hand is damaged. Depending on the cause, it can be classified into two main types: Obstetric Brachial Plexus Palsy (OBPP) and Traumatic Brachial Plexus Palsy. This guide provides an in-depth exploration of both forms, including causes, symptoms, diagnostic methods, treatment options, rehabilitation approaches, and prognosis.

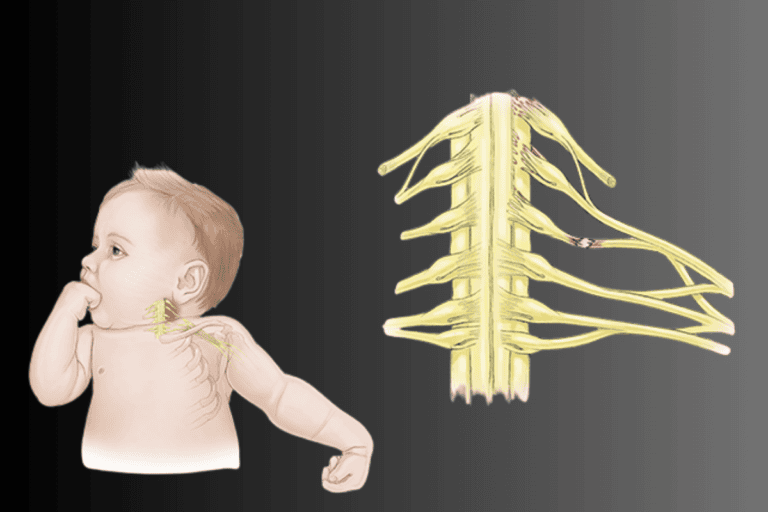
Obstetric Brachial Plexus Palsy (OBPP)
Obstetric Brachial Plexus Palsy (OBPP) occurs in newborns when the brachial plexus nerves are injured during the birth process. This type of injury typically happens during complicated deliveries, especially in cases involving large babies, prolonged labor, or breech presentations.

Types for OBPP (Newborns)
")
OBPP can be categorized based on the specific nerves affected:
1. Erb’s palsy
- Involves the upper brachial plexus (C5-C6 nerves).
- Causes weakness in the shoulder and upper arm, with limited ability to raise the arm or rotate the shoulder.
2. Klumpke’s palsy
- Involves the lower brachial plexus (C8-T1 nerves).
- Leads to weakness in the forearm, wrist, and hand, sometimes causing a claw-like hand deformity.
3. Global palsy
- Involves the entire brachial plexus, resulting in complete paralysis of the arm.
")
- Weakness or limpness in the arm.
- Limited movement of the shoulder, elbow, or hand.
- Decreased grip strength in the affected hand.
- Abnormal arm positioning (e.g., arm held close to the body with the elbow extended and wrist flexed).
- Absence of the Moro reflex on the affected side.
Causes for OBPP (Newborns)
")
OBPP is primarily caused by excessive stretching or compression of the brachial plexus nerves during childbirth. Common risk factors include:
- Shoulder dystocia: A delivery complication where the baby’s shoulder becomes stuck behind the mother’s pelvic bone after the head has been delivered.
- Breech deliveries: In breech presentations, where the baby’s buttocks or feet are delivered first, there is an increased risk of nerve injury.
- Prolonged labor: Extended labor increases the likelihood of using force during delivery, which may stretch or compress the nerves.
- Use of assisted delivery tools: The use of forceps or vacuum extractors can increase the risk of nerve damage.
Risk factors for OBPP (Newborns)
")
1. Maternal risk factors
- Gestational diabetes: Increases the likelihood of having a larger baby, which raises the risk of shoulder dystocia and subsequent nerve injury.
- Obesity: Larger mothers may face complications in labor that increase the risk of OBPP.
- Advanced maternal age: Older mothers may be at a higher risk of complications during childbirth.
2. Fetal risk factors
- Large birth weight (Macrosomia): Babies weighing more than 8 pounds, 13 ounces are at a higher risk.
- Breech presentation: Babies positioned feet-first or bottom-first during delivery are at an increased risk.
- Premature birth: Premature infants may have underdeveloped muscles and less fat, which increases their vulnerability to nerve injury.
Diagnosis for OBPP (Newborns)
")
Diagnosis typically involves a combination of clinical examination and imaging studies:
1. Clinical examination
- Observing the arm’s posture and movement.
- Checking reflexes, muscle tone, and grip strength.
2. Imaging tests
- Ultrasound: Helps assess shoulder joint alignment and detect nerve continuity.
- MRI: Provides detailed images of the brachial plexus, identifying nerve damage or compression.
3. Electrodiagnostic tests
- Nerve Conduction Studies (NCS): Measures how well and how fast electrical signals travel through the nerves.
- Electromyography (EMG): Evaluates the electrical activity of muscles to detect nerve dysfunction.
Treatment for OBPP (Newborns)
Non-surgical treatments
")
1. Physiotherapy
- Aims to maintain joint flexibility and prevent contractures.
- Involves passive range-of-motion exercises for the shoulder, elbow, wrist, and hand.
- Cons:
- May not be effective for severe nerve damage.
- Requires consistent effort over a long period.
2. Occupational therapy
- Focuses on improving fine motor skills and hand function.
- Incorporates play-based therapy to encourage movement.
- Cons:
- Progress can be slow.
- Limited benefit if nerve function is severely impaired.
3. Splinting
- Splints may be used to maintain proper joint positioning and prevent deformities.
- Cons:
- Long-term use may cause discomfort.
- Does not address underlying nerve damage.
While non-surgical treatments play a vital role in managing OBPP, they are often temporary measures aimed at preserving joint function and preventing further complications. For severe cases where there is little to no improvement within the first few months, surgical intervention remains the best option to restore nerve function and improve outcomes.
Surgical treatment
")
Surgical intervention is considered if there is no significant improvement within 3 to 6 months. Surgical options include:
1. Nerve repair
- In cases of partially torn nerves, direct repair is performed by suturing the severed ends together. This procedure is best suited for clean cuts and minor tears, where nerve continuity can be restored.
- Details:
- Typically performed under a microscope to ensure precision.
- Requires careful post-operative management to prevent scarring and adhesion formation, which could inhibit nerve regeneration.
2. Nerve grafting
- When a segment of the nerve is completely damaged or missing, a nerve graft is harvested from another part of the patient’s body (commonly the sural nerve in the leg) to bridge the gap.
- Details:
- The graft serves as a scaffold for regenerating nerve fibers to grow through.
- Recovery depends on the length of the graft and the age of the patient, as younger patients tend to have better outcomes.
- Potential donor site morbidity includes numbness or tingling at the graft harvest site.
- The graft serves as a scaffold for regenerating nerve fibers to grow through.
3. Nerve transfers
- In cases where the original nerves cannot be repaired or grafted, healthy nerves from other parts of the body are transferred to reinnervate the affected muscles.
- Details:
- Common donor nerves include the spinal accessory nerve and the intercostal nerves.
- This approach is particularly useful for restoring function in cases of avulsion injuries, where the nerve root is pulled out from the spinal cord.
- Post-operative therapy is crucial for retraining the brain to use the transferred nerves for new functions.
- Common donor nerves include the spinal accessory nerve and the intercostal nerves.
Surgical outcomes vary based on the severity of the injury, the timing of the procedure, and post-operative rehabilitation. Early intervention and meticulous surgical techniques generally yield the best results.
Rehabilitation for OBPP (Newborns)
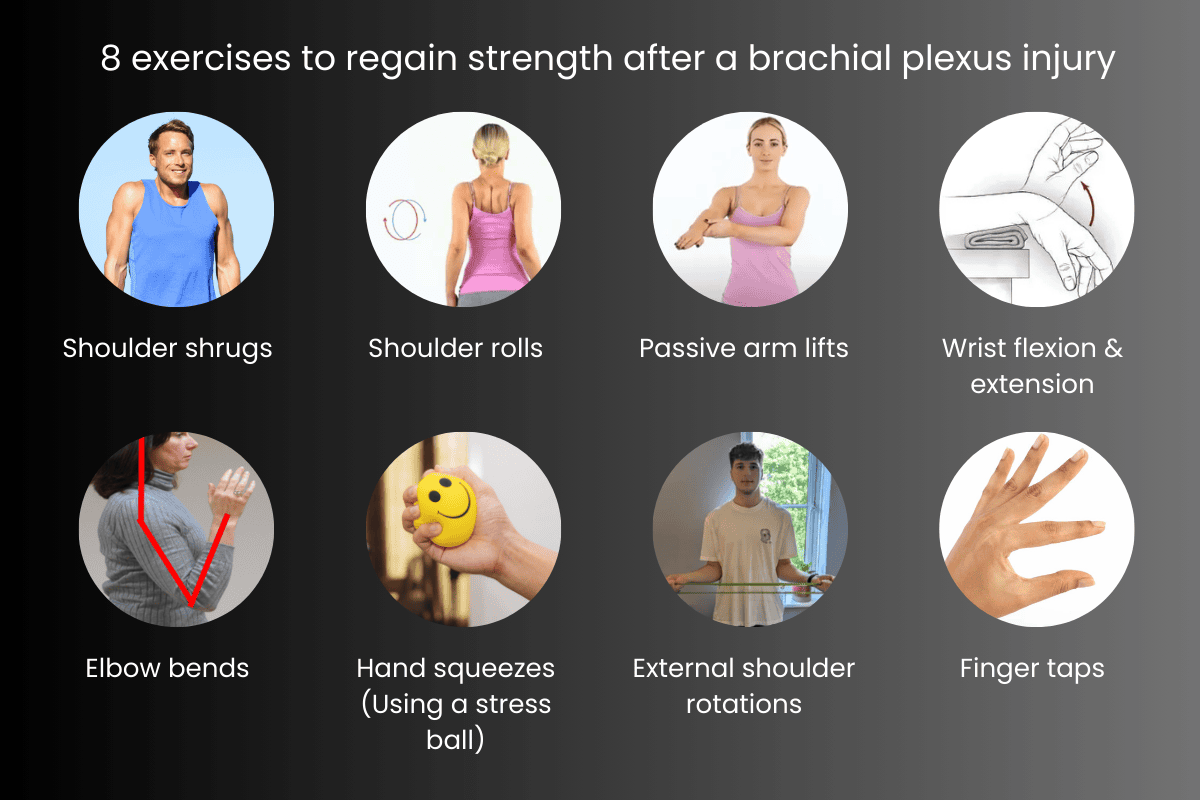
Post-treatment rehabilitation is essential for restoring arm function. Rehabilitation programs include:
- Strengthening exercises: To rebuild muscle strength.
- Sensory re-education: To retrain the brain to interpret sensations from the arm.
- Functional training: To improve coordination and the ability to perform daily activities.
Prognosis for OBPP (Newborns)
The prognosis for OBPP varies depending on the severity of the injury. Mild cases, such as neuropraxia (nerve stretching), often recover fully within a few months. More severe injuries, including nerve ruptures, may require surgical intervention and prolonged rehabilitation, with variable outcomes.
Prevention for OBPP (Newborns)
Proper delivery management:
- Careful handling during birth: Ensuring proper techniques and maneuvers during delivery (e.g., preventing shoulder dystocia) can reduce the risk of OBPP.
- Cesarean section for risky deliveries: If there are risk factors such as macrosomia or breech presentation, a cesarean section may be considered to avoid excessive stretching of the brachial plexus.
Prenatal care:
- Monitoring fetal growth: Regular prenatal check-ups to monitor fetal growth and plan for delivery based on the baby’s size can help manage risks.
- Management of maternal health: Proper control of gestational diabetes, weight management, and other health conditions during pregnancy can reduce the chances of OBPP.
Traumatic brachial plexus palsy
Traumatic Brachial Plexus Palsy occurs when the brachial plexus nerves are injured due to high-impact trauma, such as road accidents or sports injuries. This form of palsy can result in partial or complete paralysis of the arm, depending on the extent of the injury.

Types of traumatic brachial plexus injuries

1. Neuropraxia (Stretch injury)
The mildest form of injury where the nerve is stretched but not torn. Recovery typically occurs within weeks or months.
2. Axonotmesis
A more severe injury where the nerve fibers are damaged, but the outer covering remains intact. Recovery may take several months.
3. Neurotmesis (complete rupture)
The nerve is completely torn, requiring surgical repair.
4. Avulsion
The most severe form, where the nerve root is torn away from the spinal cord. Recovery is unlikely without surgical intervention.
Symptoms for traumatic brachial plexus palsy (adults)
")
- Loss of sensation or numbness in the arm.
- Weakness or paralysis of the shoulder, arm, or hand.
- Severe burning or shooting pain.
- Muscle atrophy due to prolonged nerve dysfunction.
Causes for traumatic brachial plexus palsy (adults)

Common causes of traumatic brachial plexus palsy include:
- Motor vehicle accidents: The most common cause, especially in motorcycle accidents where the shoulder is forcefully stretched.
- Sports injuries: High-impact sports like rugby, football, or wrestling can cause nerve damage.
- Falls: Sudden falls where the arm is pulled or stretched excessively.
- Penetrating injuries: Knife wounds or gunshot injuries that directly damage the brachial plexus.
- Tumors or Radiation therapy: Tumors pressing on the brachial plexus or radiation treatment in the chest region can lead to nerve damage.
Risk factors for traumatic brachial plexus palsy (adults)
")
- High-risk activities:
- Motorcycle accidents: The risk of high-impact trauma to the shoulder or neck is significant in motorcycle accidents.
- Sports injuries: Football, rugby, wrestling, and other contact sports are common causes.
- Falls: Falling from a height or in accidents, where the arm is pulled or overstretched.
- Motorcycle accidents: The risk of high-impact trauma to the shoulder or neck is significant in motorcycle accidents.
- Age: Older individuals may have reduced tissue elasticity and bone fragility, leading to more severe injuries.
- Pre-existing conditions: People with conditions like cervical spondylosis or tumors near the brachial plexus are at an increased risk of nerve compression or injury.
Diagnosis for traumatic brachial plexus palsy (adults)
")
Diagnosis of traumatic brachial plexus palsy typically involves:
- Physical examination: To assess muscle strength, sensation, and range of motion.
- Electromyography (EMG): To evaluate nerve function and pinpoint the location of the injury.
- Imaging tests: MRI or CT scans can provide detailed images of the soft tissues and nerves to evaluate the extent of injury.
Treatment for traumatic brachial plexus palsy (adults)
Non-surgical treatments

1. Physical therapy
Purpose: Physical therapy aims to preserve muscle strength, maintain joint flexibility, and improve overall arm function. Early rehabilitation is crucial to prevent muscle wasting and the development of joint stiffness.
Cons:
- Time-consuming: Rehabilitation can take months or even years, and the results may be slow.”
- Limited effectiveness in severe cases: For those with significant nerve damage or severe weakness, physical therapy alone may not restore full function.
- Requires consistency: It demands consistent effort from both the patient and therapist, and progress can be frustratingly slow in more severe cases.
2. Pain management
Purpose: Pain management involves using medications such as over-the-counter pain relievers (e.g., ibuprofen), prescription medications (e.g., opioids or nerve pain medications), or nerve blocks to control pain during recovery.
Cons:
- Temporary relief: Pain management only offers short-term relief, and does not address the underlying nerve damage.
- Side effects: Pain medications, particularly opioids, can lead to side effects such as nausea, dizziness, or dependence if used for extended periods.
- Ineffective for severe pain: In some cases, pain management alone may not be sufficient to manage the severe nerve pain that often accompanies brachial plexus injuries.
While non-surgical treatments play a vital role in managing OBPP, they are often temporary measures aimed at preserving joint function and preventing further complications. For severe cases where there is little to no improvement within the first few months, surgical intervention remains the best option to restore nerve function and improve outcomes.
Surgical treatment
When traumatic injury to the brachial plexus occurs, surgery is often required to restore function to the affected arm if non-surgical methods (like physical therapy or pain management) are ineffective. Traumatic injuries can involve various levels of nerve damage, from stretching to complete severing, which determines the appropriate surgical intervention.

1. Nerve repair
Nerve repair in traumatic brachial plexus palsy involves reconnecting or repairing the injured nerve if it is stretched, compressed, or partially severed.
- Procedure:
- Surgeons may perform a neurolysis to remove scar tissue or other compressing elements around the damaged nerve.
- If the nerve is cleanly severed or has a gap, surgeons will attempt to reattach the two ends of the nerve using microsurgical techniques and sutures. This is done as soon as possible after the injury to minimize the risk of nerve degeneration.
- Surgeons may perform a neurolysis to remove scar tissue or other compressing elements around the damaged nerve.
- Recovery:
- Nerve repair is a slow process, as nerves regrow at a rate of approximately 1 inch per month. It can take up to a year or more to fully assess the success of the repair, with regular physical therapy to support recovery.
- Nerve repair is a slow process, as nerves regrow at a rate of approximately 1 inch per month. It can take up to a year or more to fully assess the success of the repair, with regular physical therapy to support recovery.
- Success:
- The success rate depends on how soon the nerve repair is done after the injury and the extent of the damage. Earlier repairs tend to yield better functional outcomes.
2. Nerve grafting
When the traumatic injury causes extensive nerve damage or complete nerve severing, nerve grafting is employed. This involves using healthy nerves from other areas of the body to replace the damaged nerves.
- Procedure:
- Surgeons harvest healthy donor nerves from areas like the leg (sural nerve) or the neck. These nerves are selected because they are similar in structure to the brachial plexus nerves.
- The harvested nerve is carefully placed in the area where the brachial plexus nerve is damaged, and the ends are sutured into place, allowing nerve regeneration to occur.
- Surgeons harvest healthy donor nerves from areas like the leg (sural nerve) or the neck. These nerves are selected because they are similar in structure to the brachial plexus nerves.
- Recovery:
- The healing and regrowth of the nerves can take several months to a year, depending on the severity of the injury and the length of the graft. Physical therapy is essential to support recovery and maintain muscle function.
- The healing and regrowth of the nerves can take several months to a year, depending on the severity of the injury and the length of the graft. Physical therapy is essential to support recovery and maintain muscle function.
- Success:
- Nerve grafting has a good success rate when the nerves have not been completely torn beyond repair. However, the recovery of fine motor control, particularly in the hand, can be limited depending on the extent of nerve loss and the timing of the surgery.
3. Nerve transfers
Nerve transfer is a more advanced procedure used when nerve damage is too severe for repair or grafting. In traumatic cases, nerves from other parts of the body are rerouted to the injured area to restore function.
- Procedure:
- Surgeons select donor nerves that are functional but can be spared. The spinal accessory nerve, intercostal nerves, or suprascapular nerve are commonly used for this procedure.
- These nerves are re-routed and surgically connected to the damaged nerves in the brachial plexus to restore function in the shoulder, arm, or hand.
- Surgeons select donor nerves that are functional but can be spared. The spinal accessory nerve, intercostal nerves, or suprascapular nerve are commonly used for this procedure.
- Recovery:
- The recovery from nerve transfer surgery can be lengthy, taking up to a year or more. Regaining function may be gradual, and patients need extensive rehabilitation to re-educate the muscles to respond to the new nerve pathways.
- The recovery process involves physical therapy to strengthen muscles and improve motor control.
- The recovery from nerve transfer surgery can be lengthy, taking up to a year or more. Regaining function may be gradual, and patients need extensive rehabilitation to re-educate the muscles to respond to the new nerve pathways.
- Success:
- Nerve transfer surgery can be quite effective for restoring gross motor function (e.g., shoulder and elbow movements), especially when nerves are severely damaged and cannot be repaired. However, it may not fully restore fine motor skills, such as hand dexterity.
4. Muscle or Tendon transfer
In severe traumatic brachial plexus injuries, when nerve recovery is not possible or successful, muscle or tendon transfer may be performed to restore functionality to the arm.
- Procedure:
- Surgeons choose healthy muscles or tendons from other areas of the body, often from the upper thigh or forearm, and relocate them to the shoulder, elbow, or hand area to restore function to the affected limb.
- The chosen muscle or tendon is reattached to the area of the body where it is needed, with microsurgical techniques used to ensure that blood flow and nerve supply are sufficient for the new location.
- Surgeons choose healthy muscles or tendons from other areas of the body, often from the upper thigh or forearm, and relocate them to the shoulder, elbow, or hand area to restore function to the affected limb.
- Recovery:
- After muscle or tendon transfer, patients undergo extensive physical therapy to retrain the body to use the transferred muscle. This can take several months to years for full rehabilitation.
- Recovery often involves improving strength and mobility, though fine motor control may not fully return.
- After muscle or tendon transfer, patients undergo extensive physical therapy to retrain the body to use the transferred muscle. This can take several months to years for full rehabilitation.
- Success:
- Muscle or tendon transfers are effective in restoring gross motor function (e.g., lifting the arm or moving the shoulder) but generally cannot restore fine motor skills (e.g., hand movement). The overall outcome depends on the muscle or tendon chosen for transfer and the patient’s rehabilitation process.
Rehabilitation for traumatic brachial plexus palsy (adults)
Rehabilitation focuses on restoring as much function as possible:
- Strength training: To regain muscle power.
- Range of motion exercises: To maintain flexibility.
- Functional therapy: To improve daily activities and overall quality of life.
Prognosis for traumatic brachial plexus palsy (adults)
The prognosis for traumatic brachial plexus palsy depends on the severity of the injury and the timing of treatment. Early intervention offers the best outcomes, though severe injuries may result in permanent disability despite surgical treatment.
Prevention for traumatic brachial plexus palsy (adults)
Safety measures:
- Use of protective gear: Wearing helmets and other protective gear during high-risk activities like motorcycle riding or contact sports can minimize the risk of brachial plexus injuries.
- Motor vehicle safety: Proper seat belt use, along with awareness of safe driving practices, can reduce the likelihood of accidents causing nerve injury.
Strengthening muscles:
- Physical conditioning: Regular strength training and flexibility exercises can help prevent strains and injuries to the brachial plexus during physical activities or sports.
Workplace safety:
- Ergonomics: Ensuring proper posture and avoiding repetitive strain injuries in the workplace (e.g., lifting heavy objects improperly) can help reduce the risk.
What makes us the best hospital for brachial plexus palsy treatment in Ahmedabad?
We pride ourselves on providing exceptional care for patients with brachial plexus palsy. Here’s why patients across Ahmedabad trust Krisha hand hospital for their treatment:

Expertise of Dr. Karn Maheshwari
He is a highly skilled hand & wrist surgeon specialized in treating brachial plexus palsy. His specialized knowledge ensures that you receive the most effective treatment tailored to your individual needs.

Personalized treatment plans
We believe that no two patients are the same. Dr. Maheshwari tailors each treatment plan based on your specific symptoms, lifestyle, and preferences, ensuring you get the most effective and least invasive care possible.

Minimally invasive surgery
When surgery is necessary, we use the latest techniques to reduce scarring, shorten recovery times, and get you back to your daily activities faster.

Comprehensive physiotherapy
Our in-house physiotherapy team, led by Dr. Maheshwari, provides targeted rehabilitation exercises post-surgery to ensure optimal recovery and restore hand function as quickly as possible.
State-of-the-art facility
Our hospital is equipped with modern medical technologies, ensuring precise diagnostics and advanced treatment options for every patient.

Patient-centric care
From your first consultation to your follow-up care, our team is dedicated to providing a comfortable, compassionate experience. We prioritize open communication, answering all your questions and keeping you informed every step of the way.
Awards & Achievements








What our patients say about their hand treatment
Prem Singh Rathore
Hi, I am Prem, and I live in Naroda, Ahmedabad.
Let me tell you why you should choose Dr. Karn Maheshwari and why I believe he is the best in the business for forearm and hand surgeries.
At the age of 18, I broke my left hand(radius bone) in school in 2013. I remember I was in the 12th standard. It happened around teacher’s day.
I went to see a nearby orthopedic doctor who did my fracture and covered it with a plaster. So, there was no surgery involved.
When the plaster got uncovered, I saw my hand for the first time, and I wasn’t happy. It looked like my alignment(between radius and ulna bone) was messed up, and I wasn’t satisfied with the result.
Although the doctor kept giving me false hope about my hand, that it would get better with time, it never did.
So, I started consulting with other orthopedic specialists regarding the resolution for my messed-up wrist.
Until I met Dr. Karn Maheshwari, He answered all my questions, cleared all my doubts in and out regarding the possible hand surgery, and gave assurance that he’d only do the surgery, which would give me the satisfaction that I was looking forth.
And after Nine years of waiting, I was convinced that this was the guy I wanted to bet my money on. Now, after the surgery, my hand looks good.
The bone alignment is better, the wrist movement is better, and I feel like my hand strength is back.
If you or any of your relative is looking to visit Dr. Karn, feel free to go and consult with him, and I am sure you will get the result and the answers you’re looking forth.
You can thank me after the surgery. My no. is available with Dr. Karn.
Aashish thakor
Maru name Aashish Thakor Che Mara bhai ne Cricket Ramta Finger Ma Fracture Thayu tu Mane Dr. Sulay Sachdev ne tya Batava gayo Amne Dr.Karn Maheshwari No Reference aapyo hu Krisha Hospital ma Batava aavyo. Sir nu kam saru che Hospital Staff Saro che. Thank u sir 🙏😊
Hitendra Solanki
He is a very nice doctor. He has good experience and knowledge. I used to have a lot of pain in the first swelling of my right hand for years. Took medicines from many doctors. But no matter Dr. Karn Maheshwari sir is completely pain free after the operation.
Kiran Vankar
Maru name kirti kumar che.
Kakoshi.ta.shidhalur.dist.patan.
Maro left hand thumb cut thai gayo hato..
Dr.kan maheshwari & aemni team ae 5hr khub mahenat kari operation kari maro thumb fari thi joint kari aapyo.
Hu ane mara family aemna khub khub aabhari chhiae.
Dr.karn & aemno all staff bahu j sara nature na che. Aemni hospital pn bahu sari chhe.
Hu hammesh mate aemno aabhari chhu.thank u dr.karn & team
Panchal Nehal
Dr. Karn Maheshwari Sir Tandem Trasplantation of my arm after brachial plexus operation and tried to work as best as possible.
Karan Vashfoda
Maru hath Machine ma aai gyu hatu .. pachi me dr karn pase mara hath ni surgery karai Ane Mara hath ma sudharo Thai gayo che.. dr karn Maheshwari ne hu dhyanwad kru chu aemne mara hath ne bachavi didhu..
Shruti Modi
Dr.Karn Maheshwari the very nice ,cooperative and so experienced doctor and surgeon for any type of arm or hand problem … very successful too.
Two months ago my daughter was suffering with DQ problem in right hand and she couldn’t move wrist.. It was totally restricted by moving.. But in a first consultation with Dr. Karn we were so satisfied and been confident for successful surgery ..
In a moments of surgery with perfect guidance she is now absolutely fine and can do everything with the right hand.. Thanx to Dr.Karn.. and thnx to our doctor friend who suggested this cooperative and successful doctor…Thank you…
Kandarp Raval
Dr Karn is one of the most amazing doctors I have ever across. Not just a great doctor, he is a very good human being with a heart of gold. While most specialists told me I had to learn to put up with my ganglion pain, Dr Karn ensured I got rid of it through a successful surgery. His behaviour, treatment and never-give-up attitude boosts patients for a speedy recovery. He listens and addresses each of his patient’s complaint with utmost care and attention. A few adjectives that describe him are compassionate, respectful, attentive, dedicated, kind, empathetic and much more…..
Jyoti Morabia
Dr karn Maheshwari is best hand surgeon.he is polite and Very supportive Doctor.
1year ago I had the operation of carpel tunnel with him. I got very good cooperation from him. He was constantly taking care of me over the phone. So I am very satisfied with his work and nature….
Congratulations!!! Sir💐
Nandkishore Patel
One of the best hand and microsurgery Doctor in Gujarat. Visited his hospital and had a great experience getting treated by him. Also the staff members working with the doctor are very helpful after getting treated by him.
Lay Shah
Dr. Karn Maheshwari is really an expert and can tackle any hand related surgeries exceptionally well.
My grandmother had an accident and got a really deep wound on her finger. She needed immediate operation to get it treated. We got spontaneous help from Dr. Karn and he consolably explained us the complete process for the hand operation. He skillfully completed the operation and comforted my grandmother during the same.
Had really satisfactory experience during the entire procedure and she was discharged in the evening itself.
I would totally recommend Dr Karn Maheshwari.
Rajendra Acharaya
Hello, friends
My name is Rajendra Acharya, I am a resident of Bhilwara, Pur in Rajasthan. Friends, while playing cricket, my ring finger got completely broken in the middle due to a ball. For its treatment, I showed it to all places like Bhilwara, Ajmer, Jaipur and Udaipur, but no one got it. Any doctor at any place completely refused to fix it as before and said that there will be no movement in it and it will always remain straight. Then we talked to the person who met us in Ahmedabad and showed us 3-4 places there. We went to Dr. Rajendra ji Patel’s place in Navrangpura. There Dr. Rajendra ji Patel asked us to get treatment from Dr. Karan ji Maheshwari and without any delay we met Karan sir and got the operation done and in just 45 days my finger came back. as it happened
For this I thank Karan Sir very much for correcting my finger.
Dr Sudha Yadav
I had swelling and stiffness in fingers of my left hand for which I consulted Dr Karn Maheshwari. I found Dr Maheshwari to be with great expertise in his speciality. He explained to me in details everything and answered to all my queries with patience. He is highly professional with great skills and very kind and compassinate doctor. I am much better within short span of treatment. I thank Dr Maheshwari from core of my heart.
Er Avadh Patel
I am sharing my own experience. I had last finger injury of hand of them were almost amputated from distal part. I thanks to Dr. Karn maheshwari sir and his team did 2hr long surgery and made the operation successful. Right now after one and half month recovery my finger. Thanks to sir and his team
Ritesh Desai
Machine ma hath avi javani mari angli ma ghabhir ija thai ti …pela biji jagaya a operation thay pan Ema kai … Saru na thau nai ….p6i mane company na manager sir a … Dr Karn maheshwari sir no content karvyo … Tay mari surgery karvi …atyray mane ghanu saru che … finger ma movement avi gai che … Thank you Dr Karn maheshwari..all staff
Dhruv Raval
I was diagnosed with DQ in my left hand wrist, It was too painful even I try to take a paper, It was a worst condition for me , Dr. Karn sir operate me wisely, After operation my wrist was good, pain was relief , Moreover Dr. Karn and hospital staff were always quick to respond and provide advice with a personal touch.
Naresh Katara
After the operation of branchial plexus, pain in the hand and swelling have reduced. There is pain in the hand, now it is better than before.
Kajalba Vaghela
Dr karn Maheshwari sir is a best orthopaedic hand surgeon in gujrat . he treated my husband right hand finger ring surgery and result is so good after then my husband feel better good and hospital staff is very coperative and sir is very excellent hand surgen.
Amit
I hail from Sydney, Australia and had some severe wrist pain with a couple of lumps. I wasn’t able to get best medication in Sydney and ended up reading great about Dr Karn. So went to him and I had a wrist surgery done for a ganglion cyst and schwannoma(very painful) in March 2024. Technically, it should not be painful but due to some reason it was. Dr Karn did a great job in surgery and later told me that schwannoma was near my wrist bone which caused the pain. Bhavesh and Manisha were great nurses who helped me in my surgery and regular dressings. There was 1 another lady nurse and she was so helpful too.
Best part was Dr Karn asked me to keep him updated after the stitches were taken off.
Genuinely, you can’t get a better wrist surgeon than Dr Karn and his team.
Ankita Morbia
Dr karan maheswari is a best hand surgeon I had carpen tunnel surgery from him, back support is good staff is also good & polite the best thing of a Doctor is he gives enough time nd is of polite & kind nature
Thanks to Doctor & his team.
I recommend to every one .
Hardik Soni
**Outstanding Experience with Dr. Karna Maheshwari**
I recently underwent wrist surgery performed by Dr. Karna Maheshwari, and I cannot express enough how grateful I am for the care and expertise I received. From the initial consultation to the post-operative follow-ups, Dr. Maheshwari and his team were incredibly professional, compassionate, and attentive.
The surgery itself went smoothly, and Dr. Maheshwari took the time to explain each step of the procedure, alleviating my anxiety. His skill as a surgeon is remarkable, as I have experienced a significant improvement in my wrist function and pain levels.
Post-surgery, the recovery process was well-guided, with Dr. Maheshwari providing a comprehensive rehabilitation plan. I appreciated his willingness to answer all my questions and his proactive approach in managing my recovery.
Overall, I highly recommend Dr. Karna Maheshwari for anyone considering wrist surgery. His expertise and dedication to patient care make him an exceptional choice for orthopedic surgery.
Ranjita Patel
I had a injury due to cricket ball and my right thumb was fractured so I came at krisha hospital and surgery done by Dr karn Maheshwari after surgery my all movements are normal and i am fully satisfied with surgery and hospital staff was good.I highly recommended Dr karn Maheshwari for any hand related surgery.
Harshit Patadiya
I have undergone Finger amputation and it is performed by Mr. Karn Maheshwari at night around 2 am. He is really gem. He is so soft spoken and very polite. He is very much friendly too. Obviously he is super specialist in Hand Surgery, so there would no doubt about surgery. My finger is recovering very fast. His care for patient is at next level. Thanks Sir.
Rima Rajput
I am Nagji Rajput’s wife. My husband Abbarish works in healthcare. He was hit in the hand by a machine in the ongoing job. Karna Maheshwari performed the operation. And we got very good results. Thank you very much.
Patel Rajesh
Mare tendon repair dr Karn Maheshwari sir ae surgery kri and Hal Mane bavj saru che. Dr Karn Maheshwari very kind person.
Bhoomi Dhanwani
He is one of the best orthopedic surgeons i have met….i have been diagnosed with ulnocarpal impingement syndrome…he advised me to have a cast but the best thing about that is after my cast was removed i got 2 calls from his clinic to have a follow up on my condition which is the best i have reponse from a private practitioner i have ever received …
Dhwani Shah
I was having severe pain and restricted movement in my left wrist and was diagnosed with ganglionic cyst. Dr Karn Maheshwari got this operated very precisely and perfectly. It’s been a month and now i can do all my work without pain. Also the staff was throughout so supportive. Would surely recommend this hospital for the needful.
Jignesh Pathak
Most caring as well as friendly doctor. Perfact diagnosis and surgery was done for carpal tunnel syndrom. Very friendly and co operative staff. Clean and tidy hospital.
thanks.
Bhaumik Patel
All throughout my stay at Krisha hospital , we had a wonderful experience . They have the best available doctors in every field and experienced nurses too . Such a loving and caring behaviour , along with the best treatment . I would also appreciate the other subordinate staff for their prompt and efficient services … It also ranks number one as far as the cleanliness is concerned . Overall one of the best hospital in Gujarat we can be proud of . May God bless all the doctors and the entire staff to continue their amazing service to mankind forever .
Altaf Bhojani.
He Is Awesome Doctor for Hand Surgery…
I have Injury in Right Hand Index Finger While I Playing Cricket…
Ligaments Surgery is fully Successful…
Also Positive and Good Nature of Doctor..
Parth Modh
I am sharing my own experience. I had index and middle finger injury of where both of them were almost amputated from distal part. Dr. Karn sir and his team did 8hrs long surgery and made the operation successful. Right now after 1 month recovery my fingers are healed. Thanks to sir and his team
Jaesh Kodravi
Maro hath machine ma aavi gyo hato sir a surgury karya pachi hath have Saro thava avyo che moment thay che sir Ane hospital staff khub Saro che thank you
Bhavik shah
I m writing this review after about 3 months post my tendon wrist surgery done at krisha hospital by karn maheshwari sir and I can probably say he is genuinely one of the best doctors that I Have visited .
He operated my ecu tendon tear and its healing quite well now and the best part is he was always available on a phone call whenever there was any confusion
Thank you karn sir
Kuldeep sompura
Dr karn Maheshwari sir is a best orthopaedic hand surgeon in gujrat . he treated my sister left hand thumb surgery and result is so good and hospital staff is very coperative .
Kuldipsinh Vaghela
I was suffering from ganglion problem for one and a half years but even after seeing seven doctors, this problem was not resolved and I was very confused but after visiting Dr. Karn Maheshwari Saheb, my ganglion problem was discovered and it was operated by Dr. Karn Maheshwari Saheb Shri. I am very happy and healthy, the problem that I had for one and a half years was removed by Dr. Karn Maheshwari Sahib’s operation. The entire staff of Krisha Hospital is also very humane and very nice who takes full care of the patients. Thank you doctor Karn Maheshwari sir and entire staff.
ShaVrma
It’s been 5 months since my mother underwent her CTS surgery at your hospital
We’re really thankful to the Doctor and the entire team, her hand has completely recovered
There’s no pain, and the scarring on the wrist is so minimal that we can’t even notice.
Nemi Modi
Thanks to Dr. Karn and team for taking care of my husband… He had injury by cricket ball on Rt finger and was unable to do even normal movement… Operation was also difficult… Dr. Karn did New minimal surgery for that and now after 1.5 months of surgery now he is able to do total movement of That finger… We are so much thankful to such Hand surgeon at our society… You should also visit for any orthopedic issues… Best opinion best surgery best results… As a patient what we need more?
Newkumar Printry
4 -5 mahina pela machine ma hath avathi mara banne hath ni angadi kapayi gayeli dr karn maheshwari sir na tya surgery karavinr have mne ghanu saru che hal mne mne ghanu saru che krisha hospital and amno ghano abhari chu …………hand mate khub sari hospital che
Pratik Panasara
As being myself a doctor, i visited dr karn maheshwari for surgery of trigger thumb of my son. He explained me in details regarding medical condition of my child in details, regarding surgery and post-operative outcome for approx. 20-25 minutes and after surgery my child has complete improvement physically and cosmetically.. and also special thanks to entire KRISHA hospital’s staff for taking care of my son during pre-operative and immediate post-operative period..
Nidhi Phadnis Joshi
Best Orthopedic Doctor we wisited. Fast recovery and proper response. Well attending doctor.
Best attending staff.
Navinbhai Patel
My son was heavily injured in the industry accident and his fingers were heavily injured. That moment we appoint specialist for this kind of injury. He maintains situation very good and give my son very best treatment. And in this phase he constantly call us and give every advice we needed. We are very grateful for their service.
Hardikparmar111
I recently got treated by Dr. Karn Maheshwari after injuring myself while playing cricket. I am happy with the treatment and care I received. Dr. Maheshwari was great from start to finish.
He took time to explain my cricket ball injury and all the treatment options, so I always knew what was happening. He was clear and honest throughout, which made me feel comfortable and confident.
The treatment was excellent, and thanks to Dr. Maheshwari and the staff. I’m feeling much better and back to my normal activities. I highly recommend Dr. Maheshwari for hand injuries and surgeries.
Tehsin Luhar
Because of machine crush ingury my tendon was cut after that I was going at krisha hospital for further management and I was operated for tendon repair by dr karn Maheshwari and It was successfully done. I am Fully recovered after this surgery. Thanks to dr Karn Maheshwari and all hospital staff.
Hiten Thakkar
FLEXOR CARPI RADIALIS TENDON cut by glass, su first and second finger movement hampered so tendon repair surgery done by Dr. karn maheshwari sir.
Sandip Chunara
I had contacted many orthopedic doctors before, but the treatment and communication with Karn Maheshwari sir was the best for me and I liked the behavior and approach of his nursing staff and his Father also, Karn Maheshwari sir is the best in his field and I think that he walks with science and humanity together.
I am looking forward to the post-operative treatment with optimism and looking forward to get the best results.
Vd. Virendra V. Modi
Really great attention by Dr. Karn sir .. perfect diagnosis ..great advice and even advised for further… I had consulted or cricket injury….must visit clinic
Manish Jani
Amara bhai na bane hath machine ma aavi gaya hata Jena pasi ame dr rajan patel na referrals thi Krisha hospital ma aavya je dr Karn maheshwari ne batavyu jemne surgery kari and Hal have hath ma saru che amne ahiya bahu saru lagyu and hospital and staff bahu saru che
Abhay Mohta
I had vein problems in arms and legs, but the most important thing was to understand my problem, I knew Dr. Karn Maheswari through society, so I decided to take his appointment and meet him, and what I knew about him. More than that I felt better, he listened to me and my problem very carefully and then did a complete examination and gave me medicine, from which I am benefiting now. I would definitely say that anyone who has the same problem as me should definitely visit sir once…..thank you sir.
Gajendra pavra
I sent a patient she is employee in my company and had machine crush injury in left index finger and thumb was injured and we reached to krisha hospital and dr karn Maheshwari do successfull surgery. He is very kind and gentle person.
Jadeja Budhubha
Jai Mataji, I am Jadeja Rinkalba from village Makda Kutch Bhuj. About two months ago, while doing housework, I got a glass blow on the middle finger of my left hand. At that time I had a simple wound so I got it treated. After a period of 15 days my finger could not do any movement so I went to Mandvi Hospital for treatment, so I went to Bhuj Leva Patel Hospital for treatment as per doctor’s opinion. Dr. Leva Patel Hospital. From the opinion of Jadeja Divyarajsingh Dr. from Ahmedabad in Leva Patel Hospital at Bhuj. Dr. Kanan Maheshwari and Leva Patel Hospital. Anand Hirani performed the operation and took care of the finger after the operation as per his advice and the operation was successful. Today, after the operation, my finger is completely straight and it can also do movement, so I Dr. Kanan Maheshwari and Dr. I am very grateful to Anand Hirani. Thank you 😊
Salam Solanki
My son had a bike accident or I came to Krisha hospital after surgery and now my son is recovering, thank you Krisha hospital Karn sir and all staff.
Mukesh Patel
Mari wife ne lamba samay thi aangalio Ane angutha ma dukhavo thato hato .Dr Karn Saheb ne malya pehla main Ghana badha doctors ne batayu hatu gani davao lidhi pan farak na padyo.etle mein Dr Karn Saheb ne malvanu nakki karyu .Saheb e Mari wife ne tapasya pachhi kahyu k aama Dr Rutvij sir pase tame jao to saru Thai jase .Ane kharekhar Dr Rutvij sir ni davao thi farak padva lagyo .aa badal hu Dr Karn Saheb Ane Dr Rutvij Saheb no khub khub aabhar vyakt Karu chhu
Rathod Rajnikant
I got grinder crush injury or I met Dr. Karn Maheshwari sir or I got it from my surgery, I am almost fine now.
Naresh Patel
After meeting Dr. Karn my faith in humanity is multiplied by many time. My brother’s arm vaines was cut in an accident. I visited many hospitals but no one has the satisfactory reply. I lost my hope. But after few days I got Dr. Karn’s reference from my friend. He consulted my family and as we belong from village. He also made sure that we don’t get any financial burden. Today while writing this review my brother is recovered and started his normal life. The support from Dr. karn is like blessings for me.
Arvind Singh
It was indeed great pleasure to get the right surgical approach in case of my wrist fracture, I was confused for my displaced distal radius fracture of right hand about the operative procedures but the experience and confidence has brought the best, Dr. Karn Maheshwari with his skills and surgical expertise brought back the proper alignment of my hand by volar plate fixation for which I am thankfull to him and advocate other to seek his guidance for the prestigious hand
Satnarain Saini
Dr. Karn Maheshwari is the best Orthopaedics & Superspecialist in Hand & Microsurgery .
My son was suffering from Elbow pain from last one year, we consulted many Doctors. But Dr. Karn Maheshwari exactly diagnosed the problem of Snapping Elbow Syndrome ( Ulna Nerve + Medial head of Triceps) & confirmed it through MRI & sonography test. He personally guided & co-ordinated with radiology Doctors for this test. He performed surgery of Ulnar nerve transposition & muscle repair very successfully with best result. Throughout the whole treatment he guided and clarify every aspect. He is very friendly, co-operative, patient carrying, polite ,smiling face & give sufficient time to patient. My son is fully satisfied & heartedly thankful to Dr. Karn Maheshwari sir for excellent treatment and best result.
Dhaval Patel
My thumb was injured by machine by Dr karn maheshwari it was good experience..thank you sir
Ankit Patel
Krisha hospital is specialised in hand and wrist surgeries.
I was treated for my finger injury here
Dr. Karn sir is the one who saved my finger from losing its movement. Sir is calm and professional who made my fear go away.
All the staff members helped me with my every query.
Rajveer Singh
Dr. Karn maheshwari is an out or ordinarily surgeon; moreover, he is an out of ordinary human being. He sees patients as human beings and not objects of money making. He is highly competitive, compassionate and connected to the roots. he has cured few impossible looking cases. He is highly expressive and explains details to clients is great details . This gives the patient great comfort and confidence. I am extremely thankful to him and highly recommend Dr Maheshwari to anyone needing hand surgery.
Rajeshkumar Barot
Doctor Karn Maheshwari is a good doctor. My son had a finger fracture. I showed it to a big doctor but he said that 80% will be a defect. But Maheshwari showed him and told him that 90% movement will come in the finger. Many thanks to Dr. Karn Maheshwari sir for performing a normal operation and bringing him 90% movement.
Brinda desai
Prompt response was given to my child as I called before hand asking the staff for doctor’s availability, doctor Karn provided immediate attention and care to my son who had a fracture in his right hand. The staff is very supportive. My son has recovered in 30 days, he is facing no issues related to the movement of his hand and is slowly gaining strength at the fractured bone.
Nikunj Rathod
I taken online consultion appoinment at just 99 rs with krisha hospital located vaishnodevi the expriance was nice Dr karn maheshwari such good Dr with lots of knowledge ….thank you all staff and dr karn maheshwari
Chin Tan
Thank you for all the care that you have given me after my injury. You have made sure that I was always given the best care available. Your compassionate attention and professional care saved my finger. There are not enough words for me to express my appreciation. Because of your excellent care I have my finger. I will always be grateful for the additional years of life that your care has allowed me to enjoy.”
Most trusted and reliable.
Dr Jayantilal Rusat
It is said that healing begins with meeting a doctor and I found it true when I met Dr. Karn Maheshwari in Krisha Hospital. He is very sober and inteligent, expert in diagnosis and method of treatment.
I had an injury, which had created facture in my right foot’s fingers. I have been cured by treatment in Krisha hospital very economically.
I appreciate the qualities and mannerisms of paramedical and administrative staffs of Krisha hospital. I thanks Dr. Karn and all of them.
Fk Travels
My nephew is in uk .He had 2 surgery in right hand little finger in vadodara.But he is having severe sweeping and no movement.But sir gave bandage and sprint to wear in finger.recovery is good.sir nicely explain and heard the problem.
Pooja Thakkar
The service that I received from Krisha Hospital was excellent. Dr. Karn Maheshwari is an expert surgeon, he has explained me everything very clearly about my surgery, the staff was also helpful and kind. They ensured I had a smooth surgery and follow up, I am much satisfied with the post result and getting speedy recovery with the doctor’s instruction. I would highly recommend to anyone.
Nandkishore Patel
One of the best hand and microsurgery Doctor in Gujarat. Visited his hospital and had a great experience getting treated by him. Also the staff members working with the doctor are very helpful after getting treated by him.
Nikky Patel
Best Doctor for Hand surgery He is very good person for nature wise very polite,also gives true information for every patient and every time connecting patient for every situation
Arman Khan
Pela nana ma 7age ni umar ma te padi gya hta ane hath fekcher thayi gyu hatu pachi have 38umar ni vakhate khabar padyo ke hath no opresen karovu padse to ame Ahmadabad ma krisha hospital ma opresen karva layi gya ane opresen safal rahyo
Manjeet Singh
Really Thx Dr. Karn Maheshwari Sir and krisha hospital Ahmedabad. My child 2 yr. old and his right Hand ring Finger total ring finger total damage. but after successfully surgery done Dr. Karn Maheshwari and now Ring proper Good Conditions and proper movement Ring Finger.. Again thx Dr. Karn Maheshwari & and krisha hospital.
Dr. Karn Maheshwari is only one finger specialist he is save many people and child Finger and Hand.
Bhavesh Mehta
Dr. Karn Maheshwari is an expert surgeon. My mother gone through hand surgery and she is very much satisfied with the Surgery as the problem is completely solved. Krisha hospital has all the facilities in hospital .. Even the staff is also very kind and supportive.. will definitely suggest if you have any problems with your hands ..
Hardik Patel
Very cool Dr., Explains in details, spends time on queries raised by patients or their families. No wrong advice, will do operation only if required. Reasonable charges. My wife had to under go wrist surgery through him which was one of the very rare preiser disease, he simplified operation and tried to save wrist bones. Now she is getting better day by day. All the best Dr. Karn for your bright future.
Vipin kashyap
One of the best superspecialíst Hand surgeon. I had done my mom’s surgery and the results are way too good. I was fed up with the problem in mom’s hand and got the best resolution at Krisha Hospital
Sudha iyer dsouza
Prompt diagnosis and all possible lines of treatment were explained elaborately by Dr Karn Maheshwari. The paramedics and other staff members were very polite, considerate and helpful. Both pre-op and post-op responses from the doctor and his team have been excellent. Thank you.
Mada Bhai
Mara bhai Hamir Rabari no accident 3 mahina pahela thayo hato. Jema dabo hath Kam nato karto. Karn Maheshwari sire mast operation Kari apyu 6e. Ame temna abhari 6ia. Staff pan Saras 6e. Hospital ma khavani temaj rahevani suvidha pan Saras 6e. Abhar.
Bhimji Ahir
Dr. Thank you very much Karn Maheshwari. The hand operation done by Dr Sir was very successful. Today my brother’s hand is working perfectly. We will be thankful to him for giving him a hand operation for very little money. Dr Karn Maheshwari is very helpful for common people. I pray to Lord Krishna that Dr. Karn Maheshwari Sir may make great progress in life.
Pankaj Bhanderi
The services that I received from Dr. Karn Maheshwari is excellent. He done treatment for hand fracture of my 4 years old daughter. Dr. Karn Maheshwari and the staff are very friendly and supportive. Received perfect treatment with very much satisfactory result.
Ramesh Thanth
My name is Rameshbhai my wife was suffering from pain in wrist and hand for a long time and I got the address of Krisha hospital Dr. Karn Maheshwari I came there and operated on her now she is very well
Daya sondarva
I really like your services n after your treatment ,I m completely recovered from my fracture n now able to move my left hand properly.all staff work also liked by me.thank u so much sir for surgery of my left hand.
Zishan Iproliya
I had my operation of right elbow here and I have seen massive improvement in my range of motion which was restricted and doctor provided us with regular checkups after the surgery.
Hiren Patel
Ketan katharotiya
Dr.karn is the best hand surgeon and microsurgeon in gujarat ahmedabad.
Jignesh galsar
Doctor have good nature and my broken finger fixed very quickly with his treatment …..love the nature of staff too ….
Nidhi Patel
Dr.karn maheshwari is best hand,wrist and micro surgeon his hospital’s cleaning is best and staff nature is very good and sincerely
Hear patient sharing their experience of brachial plexus palsy treatment


- B-201, 2nd Floor, Shaligram Lakeview, Nr Vaishnodevi Circle, S.P. Ring Road, Highway, Service Rd, Vaishnodevi, Zundal, Ahmedabad, Gujarat 382421
- Mon–Sat: 11:00 AM – 01:00 PM, 06:00 PM – 08:00 PM
Every 2nd Saturday of the Month: 9:30 AM –11:00 AM - +91 75677 63301
- Sun: Closed
Emergency: 24/7 Available
FAQs about brachial plexus palsy
We provide a comprehensive range of services for Brachial Plexus Palsy, including early diagnosis, non-surgical treatments (such as physical therapy and splinting), and advanced surgical interventions like nerve grafting, nerve transfer, and muscle or tendon transfers. Our team focuses on restoring arm function and alleviating pain.
To schedule an appointment, you can call our hospital directly or book online. Our staff will guide you through the process and provide you with all the necessary information.
During your first consultation, our specialist will conduct a detailed examination, review your medical history, and assess your symptoms. Depending on the severity of the condition, additional diagnostic tests such as MRI or nerve conduction studies may be performed to determine the best treatment approach.
It’s recommended to bring a list of any current medications, a record of your symptoms, and relevant medical reports, including previous imaging or test results. This will help our specialists provide a more accurate diagnosis and tailored treatment plan.
Yes, we accept various insurance plans. It is advisable to check with your insurance provider for specific coverage details related to consultations, diagnostic tests, and treatments for Brachial Plexus Palsy.
Recovery after surgery can vary depending on the extent of nerve damage and the type of surgery performed. Generally, you can expect some improvements within a few weeks, but full recovery may take several months. A personalized rehabilitation plan will be created to support your healing.
Yes, we provide specialized physiotherapy services as part of our rehabilitation program for brachial plexus palsy. Our expert physiotherapists design personalized plans to improve strength, mobility, and arm function.
While many non-surgical treatments, such as splinting or physical therapy, may be offered on the same day as your consultation, more complex interventions like surgery typically require separate appointments. We will discuss your treatment options during the consultation.
Wait times for surgery can vary depending on factors such as the urgency of your case and our surgical schedule. During your consultation, our team will inform you about the estimated wait time based on your condition.
We offer several diagnostic tests, including MRI scans, nerve conduction studies, electromyography (EMG), and ultrasounds. These tests help evaluate the extent of nerve damage and guide the treatment plan.
Yes, before surgery, you may be advised to avoid smoking, alcohol, and blood-thinning medications, as these can affect the healing process. Our surgical team will provide specific pre-operative instructions tailored to your needs.
At Krisha hand hospital, patient safety is our top priority. We follow strict protocols, including comprehensive pre-operative assessments, advanced sterilization techniques, and vigilant monitoring during and after surgery to ensure a safe and successful procedure.
Most brachial plexus palsy surgeries are performed on an outpatient basis, meaning you can go home the same day. However, if there are any complications or special considerations, you may be required to stay overnight for observation.